
Assay Format
PBL’s VeriKine High Sensitivity Human IL-22 ELISA (Catalog No. 41701-1) has a 96 well plate coated with IL-22 capture antibody. The detection antibody is a biotinylated secondary antibody, followed by streptavidin conjugated to horseradish peroxidase (HRP) step where TMB (Tetramethylbenzidine) serves as a substrate.
The total length of the assay is 4 hours, with 0.78 - 50 pg/ml calibration range and <1 pg/ml LOQ. It accurately quantitates sub picogram levels of endogenous IL-22 in healthy human donor serum (HDS) & plasma (HDP) samples. IL-22 standard has been expressed in Human Embryonic Kidney (HEK-293) cells. Detailed studies were performed to assess the accuracy, sensitivity and robustness of this kit.
Results
Figure 1. Typical Standard Curves
Image
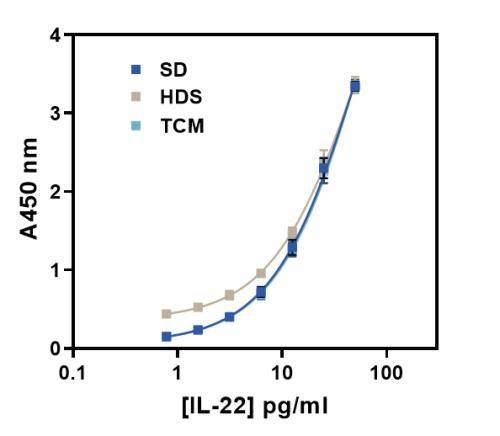
Typical Standard Curves in SD, HDS & TCM are shown. Standard diluent (SD) and TCM curves overlap, but HDS curve is shifted. The shift is due to the endogenous IL-22 (quantified separately), in the HDS sample which results in a vertical A-450 nm displacement through-out the HDS curve. Data shown is a mean of nine runs, run in triplicate. IL-22 recoveries for all matrices ranged 100% ± 20% (data not shown).
Figure 2. Spike Recovery
Image
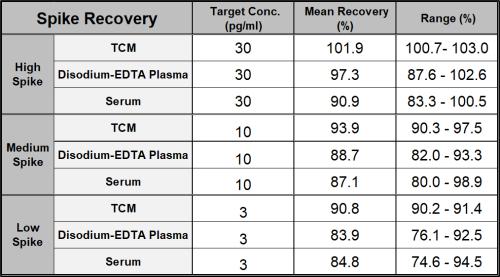
Spike Recovery TCM (n=2), Plasma (n=6) & Serum (n=5) samples were spiked with IL-22 standard at High, Medium & Low target concentrations. The table shows the mean IL-22 recovery for each sample matrix (83.9 – 101.9%).
Figure 3. Precision Studies
Image
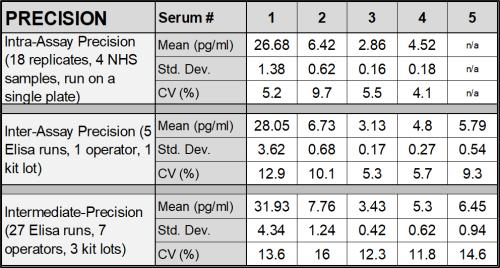
Intra-assay, Inter-assay & Intermediate precision for PBL’s ELISA kit is summarized in the table above. Single serums or Serum Pool with varying endogenous IL-22 levels were used for this study.
Figure 4 & 5. Endogenous Dilution Linearity
Image
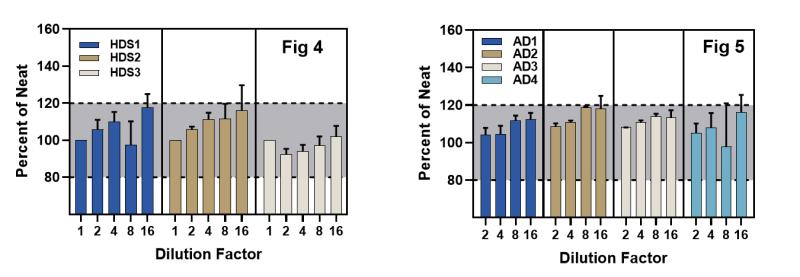
Endogenous Dilution Linearity on three HDS samples with high endogenous IL-22 and four Atopic Dermatitis (AD) diseased state sera (~18-28 pg/ml) is shown. All samples were diluted 2-fold in the standard diluent and percent recoveries calculated after adjusting for the fold dilution.
Recovery for all samples was recorded largely within 100 ± 20% of the neat value.
Error bars indicate the standard deviation between the replicates.
Figure 6. IL-22BP Inhibits the Free Protein IL-22 Standard Curve.
Image
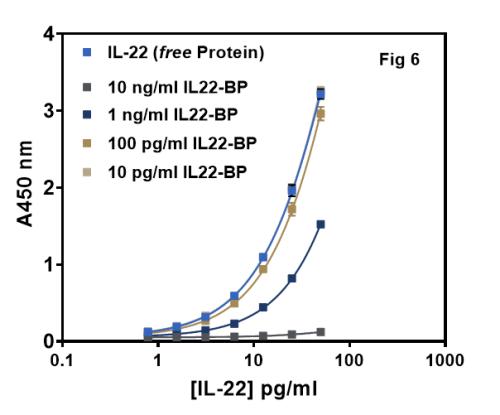
Standard curves were prepared in standard diluent (SD) with & without IL22-BP. Graph shows that 1-10 ng/ml of soluble IL-22BP added to the IL-22 SD curve, interferes with free IL-22 detection. But, at <100 pg/ml IL22-BP there is no interference in IL-22 detection. Thus, it can be concluded that PBL ELISA detects free IL-22.
Figure 7. Standard Curve Recovery
Image
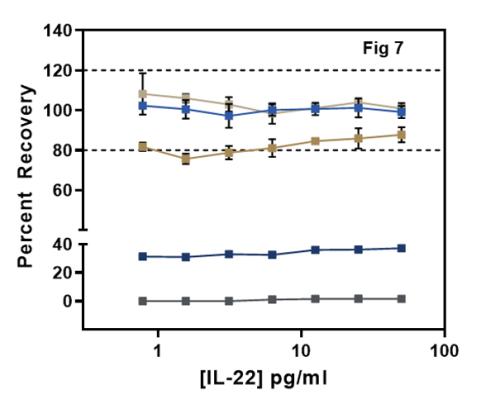
Standard Curve Recovery from Fig 6 is shown. IL-22 BP at <100pg/ml added to the IL-22 SD curve recovered IL-22 largely in the desirable range 100% ± 20%. But at higher IL-22 BP levels (1-10 ng/ml), only <40% of free IL-22 was recovered.
All curves were backfitted to the control IL-22 standard curve (free protein) in SD without any IL-22BP.
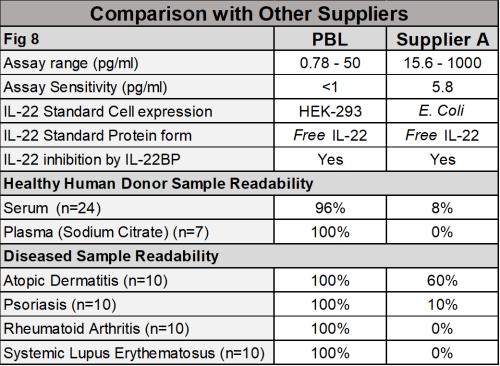
Figure 8. Performance Comparison to IL-22 Kit from Another Supplier
Image
Figures 9 & 10. PBL vs Supplier A' Standard Curves & Percent Recovery
Image
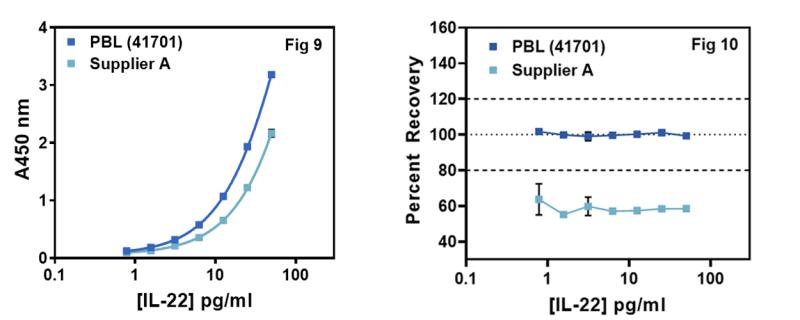
IL-22 standards of PBL and Supplier A’ were run on the PBL kit (41701-1). Graph shows the absorbance values and dose response curves in standard diluent. Supplier A’s standard exhibits a lower dose response as compared to the PBL’s standard.
The Percent Recovery of IL-22 from Fig 9 is shown. Supplier A’s E Coli IL-22 standard was backfitted against PBL’s HEK IL-22 standard. PBL’s standard shows a desirable recovery (100% ± 20%) while Supplier ‘A’ had a recovery <80%.
Figure 11. Healthy and Disease Sample Readability
Image
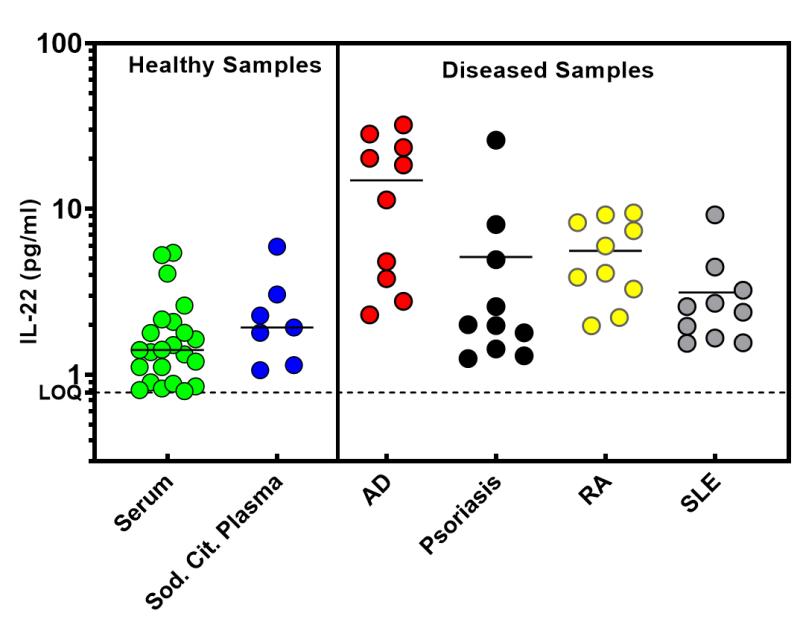
Low IL-22 levels in Healthy Donor Serum/Plasma samples were reproducibly quantified in 1-10 pg/ml range. LOQ for PBL’s kit = 0.78 pg/ml. Similarly, a few relevant Diseased state samples were quantified as shown & also summarized in Fig 8 table, such as - Atopic Dermatitis (AD), Psoriasis, Rheumatoid Arthritis (RA) and Systemic Lupus Erythematosus (SLE). All samples were tested in duplicate.
Figure 12. Healthy Donor Sample Readability Correlation
Image
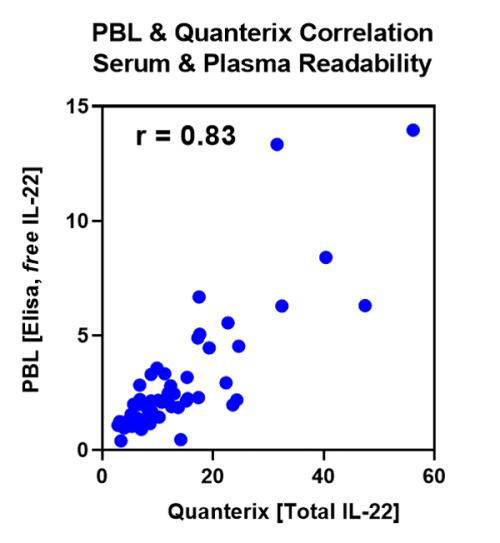
Healthy donor sample readability correlation r = 0.83 between PBL & ‘Quanterix’ is shown. ‘Quanterix’ uses SIMOA, a bead-based technology and is a pioneer in business with serum & plasma detectability in ‘femtogram’ range. Two different technologies, but similar results between the two suppliers validates the accuracy of PBL’s Elisa kit to measure free IL-22 in the similar range as ‘Quanterix’ (Total IL-22 = free + receptor bound). IL-22 in healthy human donor samples is in 1-10 pg/ml range.
Summary
PBL’s VeriKine High Sensitivity Human IL-22 ELISA (Catalog No. 41701-1) has an IL-22 standard expressed in HEK-293 cells. The high affinity form of IL-22 binding protein (IL22-BP) inhibits the measurement of free IL-22 protein at >100 pg/ml IL-22BP concentrations, suggesting that our ELISA may measure free IL-22. PBL’s kit accurately quantitates IL-22 in Healthy Human Donor Serum & Plasma and Tissue Culture Media.
Key Takeaways:
- PBL’s IL-22 ELISA calibration range is 0.78 - 50 pg/ml and <1 pg/ml LOQ. IL-22 standard of this kit is expressed in HEK-293 cells.
- Endogenous IL-22 in 100% healthy human donor serum & plasma samples was reliably and reproducibly quantitated in the expected 1-10 pg/ml range (Fig 11, 12). Similarly, 100% of the relevant Diseased state samples were quantifiable in PBL’s kit (Fig 8, 11).
- Excellent correlation between ‘PBL’ and ‘Quanterix’ (r = 0.83) further validated, accurate IL-22 measurements by the PBL’s kit. Two suppliers, two different technologies, yet similar results (Fig 12).
- Endogenous IL-22 dilution linearity (Fig 4, 5) and Precision studies (Fig 3) further confirmed the performance of this kit. Rigorous validation of this kit was done to test for sensitivity, accuracy and reproducibility.
- Spiked IL-22 recovery in complex matrices such as healthy human donor serum & plasma and TCM samples was also recorded in the desirable 100 ± 20% range (Fig 2).
References
1. Dumoutier, L., et al. 2000. Genes & Immunity. 1(8): 488-94.
2. Dudakov J., Hanash A., van den Brink, M. 2015. Annual Review of Immunology. 33: 747-785.
3. Eyerich, K., Dimartino, V., Cavani, A. 2017. European Journal of Immunology. 47(4): 607-614.
4. Eyerich, S., et al. 2017. Allergologie Select. 1(1): 71-76.
Assay Format
PBL’s VeriKine High Sensitivity Human IL-22 ELISA (Catalog No. 41701-1) has a 96 well plate coated with IL-22 capture antibody. The detection antibody is a biotinylated secondary antibody, followed by streptavidin conjugated to horseradish peroxidase (HRP) step where TMB (Tetramethylbenzidine) serves as a substrate.
The total length of the assay is 4 hours, with 0.78 - 50 pg/ml calibration range and <1 pg/ml LOQ. It accurately quantitates sub picogram levels of endogenous IL-22 in healthy human donor serum (HDS) & plasma (HDP) samples. IL-22 standard has been expressed in Human Embryonic Kidney (HEK-293) cells. Detailed studies were performed to assess the accuracy, sensitivity and robustness of this kit.
Results
Figure 1. Typical Standard Curves
Typical Standard Curves in SD, HDS & TCM are shown. Standard diluent (SD) and TCM curves overlap, but HDS curve is shifted. The shift is due to the endogenous IL-22 (quantified separately), in the HDS sample which results in a vertical A-450 nm displacement through-out the HDS curve. Data shown is a mean of nine runs, run in triplicate. IL-22 recoveries for all matrices ranged 100% ± 20% (data not shown).
Figure 2. Spike Recovery
Spike Recovery TCM (n=2), Plasma (n=6) & Serum (n=5) samples were spiked with IL-22 standard at High, Medium & Low target concentrations. The table shows the mean IL-22 recovery for each sample matrix (83.9 – 101.9%).
Figure 3. Precision Studies
Intra-assay, Inter-assay & Intermediate precision for PBL’s ELISA kit is summarized in the table above. Single serums or Serum Pool with varying endogenous IL-22 levels were used for this study.
Figure 4 & 5. Endogenous Dilution Linearity
Endogenous Dilution Linearity on three HDS samples with high endogenous IL-22 and four Atopic Dermatitis (AD) diseased state sera (~18-28 pg/ml) is shown. All samples were diluted 2-fold in the standard diluent and percent recoveries calculated after adjusting for the fold dilution.
Recovery for all samples was recorded largely within 100 ± 20% of the neat value.
Error bars indicate the standard deviation between the replicates.
Figure 6. IL-22BP Inhibits the Free Protein IL-22 Standard Curve.
Standard curves were prepared in standard diluent (SD) with & without IL22-BP. Graph shows that 1-10 ng/ml of soluble IL-22BP added to the IL-22 SD curve, interferes with free IL-22 detection. But, at <100 pg/ml IL22-BP there is no interference in IL-22 detection. Thus, it can be concluded that PBL ELISA detects free IL-22.
Figure 7. Standard Curve Recovery
Standard Curve Recovery from Fig 6 is shown. IL-22 BP at <100pg/ml added to the IL-22 SD curve recovered IL-22 largely in the desirable range 100% ± 20%. But at higher IL-22 BP levels (1-10 ng/ml), only <40% of free IL-22 was recovered.
All curves were backfitted to the control IL-22 standard curve (free protein) in SD without any IL-22BP.
Figure 8. Performance Comparison to IL-22 Kit from Another Supplier
Figures 9 & 10. PBL vs Supplier A' Standard Curves & Percent Recovery
IL-22 standards of PBL and Supplier A’ were run on the PBL kit (41701-1). Graph shows the absorbance values and dose response curves in standard diluent. Supplier A’s standard exhibits a lower dose response as compared to the PBL’s standard.
The Percent Recovery of IL-22 from Fig 9 is shown. Supplier A’s E Coli IL-22 standard was backfitted against PBL’s HEK IL-22 standard. PBL’s standard shows a desirable recovery (100% ± 20%) while Supplier ‘A’ had a recovery <80%.
Figure 11. Healthy and Disease Sample Readability
Low IL-22 levels in Healthy Donor Serum/Plasma samples were reproducibly quantified in 1-10 pg/ml range. LOQ for PBL’s kit = 0.78 pg/ml. Similarly, a few relevant Diseased state samples were quantified as shown & also summarized in Fig 8 table, such as - Atopic Dermatitis (AD), Psoriasis, Rheumatoid Arthritis (RA) and Systemic Lupus Erythematosus (SLE). All samples were tested in duplicate.
Figure 12. Healthy Donor Sample Readability Correlation
Healthy donor sample readability correlation r = 0.83 between PBL & ‘Quanterix’ is shown. ‘Quanterix’ uses SIMOA, a bead-based technology and is a pioneer in business with serum & plasma detectability in ‘femtogram’ range. Two different technologies, but similar results between the two suppliers validates the accuracy of PBL’s Elisa kit to measure free IL-22 in the similar range as ‘Quanterix’ (Total IL-22 = free + receptor bound). IL-22 in healthy human donor samples is in 1-10 pg/ml range.
Summary
PBL’s VeriKine High Sensitivity Human IL-22 ELISA (Catalog No. 41701-1) has an IL-22 standard expressed in HEK-293 cells. The high affinity form of IL-22 binding protein (IL22-BP) inhibits the measurement of free IL-22 protein at >100 pg/ml IL-22BP concentrations, suggesting that our ELISA may measure free IL-22. PBL’s kit accurately quantitates IL-22 in Healthy Human Donor Serum & Plasma and Tissue Culture Media.
Key Takeaways:
- PBL’s IL-22 ELISA calibration range is 0.78 - 50 pg/ml and <1 pg/ml LOQ. IL-22 standard of this kit is expressed in HEK-293 cells.
- Endogenous IL-22 in 100% healthy human donor serum & plasma samples was reliably and reproducibly quantitated in the expected 1-10 pg/ml range (Fig 11, 12). Similarly, 100% of the relevant Diseased state samples were quantifiable in PBL’s kit (Fig 8, 11).
- Excellent correlation between ‘PBL’ and ‘Quanterix’ (r = 0.83) further validated, accurate IL-22 measurements by the PBL’s kit. Two suppliers, two different technologies, yet similar results (Fig 12).
- Endogenous IL-22 dilution linearity (Fig 4, 5) and Precision studies (Fig 3) further confirmed the performance of this kit. Rigorous validation of this kit was done to test for sensitivity, accuracy and reproducibility.
- Spiked IL-22 recovery in complex matrices such as healthy human donor serum & plasma and TCM samples was also recorded in the desirable 100 ± 20% range (Fig 2).
References
1. Dumoutier, L., et al. 2000. Genes & Immunity. 1(8): 488-94.
2. Dudakov J., Hanash A., van den Brink, M. 2015. Annual Review of Immunology. 33: 747-785.
3. Eyerich, K., Dimartino, V., Cavani, A. 2017. European Journal of Immunology. 47(4): 607-614.
4. Eyerich, S., et al. 2017. Allergologie Select. 1(1): 71-76.
